Scoliosis is a term used to describe a curvature of the spine that is not “normal.” The normal curves of the spine include an inward curve in the low back and neck and an outward curve in the mid-back when looking at the person from the side (“sagittal plane”). However, there should NOT be any curves when looking at a person from the front or back (the frontal plane); the spine should be straight. When there is a curve in the frontal plane, this is called scoliosis and it’s usually either a singe curve, shaped like the letter “C” or a double (or more) curve, shaped like the letter “S”. Though there is a diagnostic code specific for scoliosis, it is not in itself a disease or a diagnosis and frequently, there are no or at worst, minimal symptoms associated with it. For this reason, most of the time, scoliosis is not noticed until the curve progresses significantly and a friend or family member makes a comment about it or a school screening picks it up.
The most common spinal location for scoliosis to develop is in the middle to upper back (called the thoracic spine) but it can also be located at the junction between the mid back and low back, as well as in the low back only or more rarely, in the neck only. Since there are rarely symptoms associated with scoliosis, the way it’s found is by observing one or more of the following:
- One shoulder is higher than the other
- One shoulder blade sticks out more than the other
- One side of the rib cage appears higher than the other (called a “rib hump”)
- One hip appears higher or more prominent than the other
- The waist appears uneven
- The body tilts to one side
- One leg may appear or actually be shorter than the other
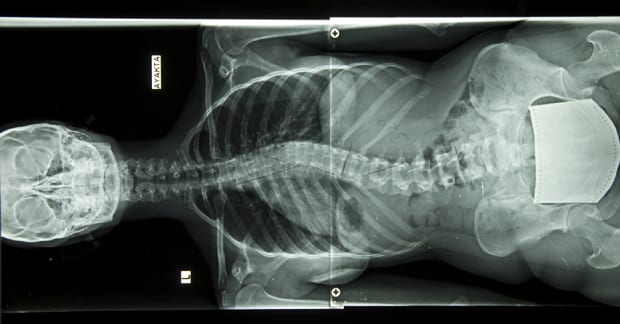
The use of X-ray usually is appropriate to confirm the diagnosis and to measure the amount of curve, which can then be used for future comparison and to rule out a possible unusual cause of scoliosis. Rarely is an MRI required – only in cases where neurological signs and symptoms exist and in younger children (ages 8-11 years old) as scoliosis almost always occurs during the puberty time frame when hormonal systems are kicking in, such as ages 12-14. When scoliosis occurs at ages less than 11, when there are neurological changes (reflex, muscle strength, and/or sensory functions), and/or when the mid-back/thoracic curve bends to the left (as it almost always curves to the right), an MRI is appropriate to rule out spinal cord pressure.
The decision to treat or not to treat is dependent on 2 factors: 1) the “skeletal maturity of the patient” (how much growing is left for the person); 2) the degree of the curve. In general, the bigger the curve and the younger the patient, the greater the chance for curve progression or worsening. With that said, curves less 10° reportedly don’t require treatment but over 20° should be watched at 4-6 month intervals. If a curve progresses >5° and/or when the curve is >30° in an adolescent, the person should be treated – most doctors would utilize a back brace. Chiropractors can offer additional care by applying spinal adjustments, reducing leg length deficiencies when a compensatory lumbar/low back curve is present, and by offering scoliosis-specific exercises.
Thousands of Doctors of Chiropractic across the United States and Canada have taken "The ChiroTrust Pledge":
“To the best of my ability, I agree to
provide my patients convenient, affordable,
and mainstream Chiropractic care.
I will not use unnecessary long-term
treatment plans and/or therapies.”
To locate a Doctor of Chiropractic who has taken The ChiroTrust Pledge, google "The ChiroTrust Pledge" and the name of a town in quotes.
(example: "ChiroTrust Pledge" "Olympia, WA")
Content Courtesy of Chiro-Trust.org. All Rights Reserved.